from Ob/Gyn & Women’s Health – Medscape https://www.medscape.com/viewarticle/insomnia-boosts-depression-risk-after-breast-cancer-2025a1000uka?src=
via IFTTT
Chlorohydrin 3-MCPD in Bragg’s Liquid Aminos
Chlorohydrin contaminates hydrolyzed vegetable protein products and refined oils.
In 1978, chlorohydrins were found in protein hydrolysates. What does that mean? Proteins can be broken down into amino acids using a chemical process called hydrolysis, and free amino acids (like glutamate) can have taste-enhancing qualities. That’s how inexpensive soy sauce and seasonings like Bragg’s Liquid Aminos are made. This process requires high heat, high pressure, and hydrochloric acid to break apart the protein. The problem is that when any residual fat is exposed to these conditions, it can form toxic compounds called chlorohydrins, which are toxic at least to mice and rats.
Chlorohydrins like 3-MCPD are considered “a worldwide problem of food chemistry,” but no long-term clinical studies on people have been reported to date. The concern is about the detrimental effects on the kidneys and fertility. In fact, there was a time 3-MCPD was considered as a potential male contraceptive because it could so affect sperm production, but research funding was withdrawn after “unacceptable side effects [were] observed in primates.” Researchers found flaccid testes in rats, which is what they were going for, but it caused neurological scars in monkeys.
What do you do when there are no studies in humans? How do you set some kind of safety factor? It isn’t easy, but you can take the lowest observed adverse effect level (LOAEL) in animal studies, which, in this case, was kidney damage, add in some kind of fudge factor, and then arrive at an estimated tolerable daily intake (TDI). For 3-MCPD, this means that high-level consumers of soy sauce may exceed the limit. This was based on extraordinarily high contamination levels, though. Since that study, Europe introduced a regulatory limit of 20 parts per billion (ppb) of 3-MCPD in hydrolyzed vegetable protein products like liquid aminos and soy sauce. The U.S. standards are much laxer, though, setting a “guidance level” of up to 50 times more, 1,000 parts per billion.
I called Bragg’s to see where it fell, and the good news is that it is doing an independent, third-party analysis of its liquid aminos for 3-MCPD. The bad news is that, despite my pleas that it be fully transparent, Bragg’s wouldn’t let me share the results with you. I have seen them, though, but I’m only allowed to confirm they comfortably meet the U.S. standards but fail to meet the European standards.
This is just the start of the 3-MCPD story, though. A study in Italy tested individuals’ urine for 3-MCPD or its metabolites, and 100% of the people turned up positive, confirming that it’s “a widespread food contaminant.” But 100% of people aren’t consuming soy sauce or liquid aminos every day. Remember, the chemical results from a reaction with residual vegetable oil. When vegetable oil itself is refined, when it’s deodorized and bleached, those conditions also lead to the formation of 3-MCPD.
Indeed, we’ve known for years that various foods are contaminated. In what kinds of foods have these kinds of chemicals been detected? Well, if they’re in oils and fats, then they’re in greasy foods made from them: margarine, baked goods, pastries, deep-fried foods, fatty snacks like potato and corn chips, as well as infant formula.
The U.S. Food and Drug Administration’s limit for soy sauce is 1,000 ppb, but donuts can have more than 1,200 ppb, salami more than 1,500 ppb, ham nearly 3,000 ppb, and French fries in excess of 6,000 ppb, as seen here and at 4:03 in my video The Side Effects of 3-MCPD in Bragg’s Liquid Aminos.
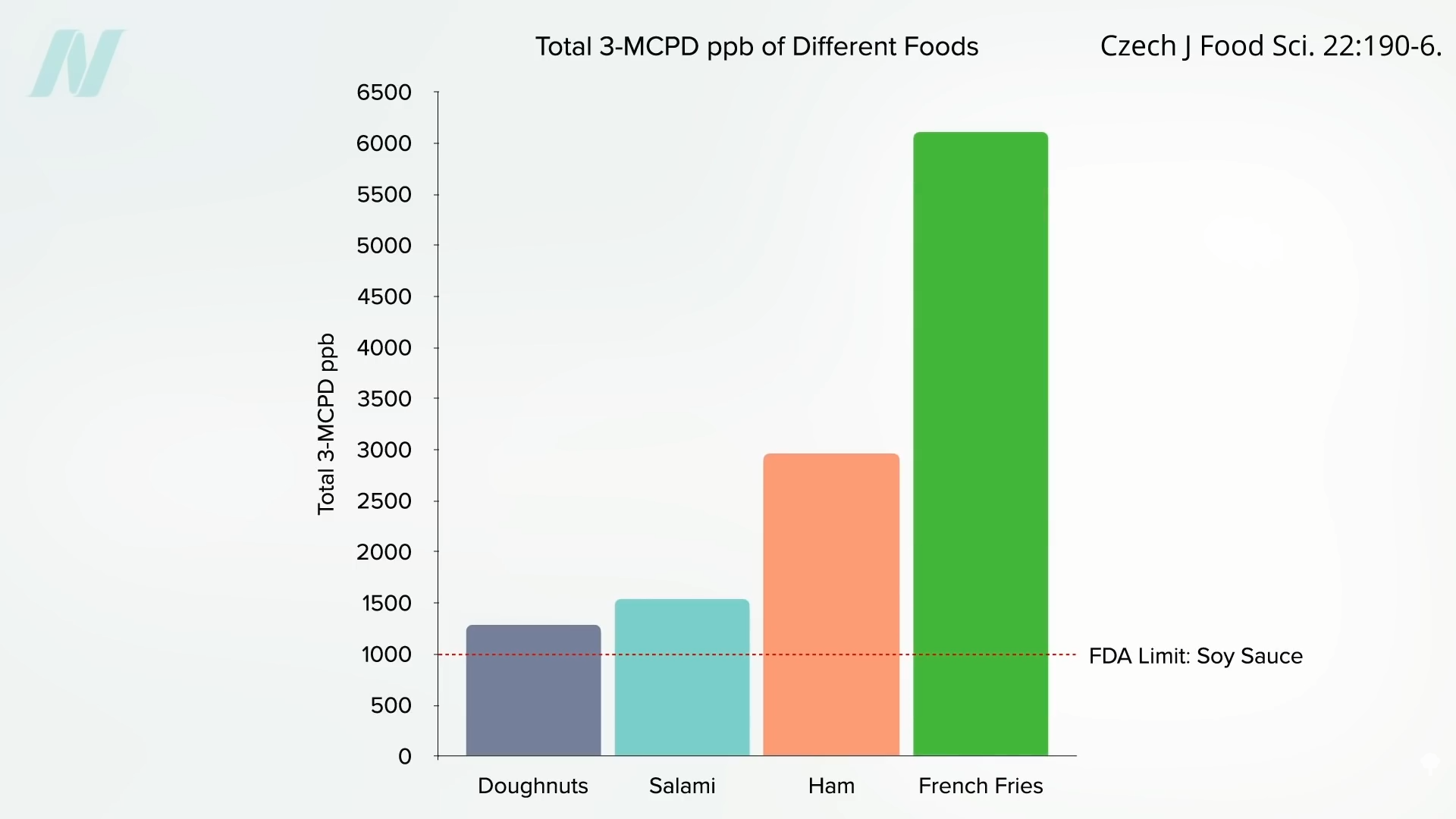
Most of us don’t have to worry about this problem, unless we’re consumers of fried food. Someone weighing about 150 pounds, for example, who eats 116 grams of donuts, would exceed the European Food Safety Authority’s TDI, even if those donuts were the person’s only source of exposure. That’s about two donuts, but the same limit-blowing amount of 3-MCPD could be found in only five French fries.
Doctor’s Note
Believe me, I pleaded with the Bragg’s folks over and over. It’s curious to me that Bragg’s allowed me to talk about where its level of 3-MCPD fell compared to the standards but not say the number itself. At least it’s doing third-party testing.
Learn more about this topic in my video 3-MCPD in Refined Cooking Oils.
You can also check out Friday Favorites: The Side Effects of 3-MCPD in Bragg’s Liquid Aminos and Refined Cooking Oils.
from NutritionFacts.org https://nutritionfacts.org/blog/chlorohydrin-3-mcpd-in-braggs-liquid-aminos/
via IFTTT
Just a moment…
from Ob/Gyn & Women’s Health – Medscape https://www.medscape.com/viewarticle/rural-high-poverty-areas-rely-most-international-physicians-2025a1000ty8
via IFTTT
Treat the Cause
Treat the underlying cause of chronic lifestyle diseases.
It’s been said that more than 2,000 years ago, Hippocrates declared, “Let food be thy medicine and medicine be thy food.” In actuality, it appears that he never actually said those words, but there’s “no doubt about the relevance of food…and its role in health and disease states” in his writings. Regardless, 2,000 years ago, disease was thought to arise from a bad sense of “humors,” as you can see here and at 0:32 in my video Lifestyle and Disease Prevention: Your DNA Is Not Your Destiny.
Now, we have science, and there is “an overwhelming body of clinical and epidemiological evidence illustrating the dramatic impact of a healthy lifestyle on reducing all-cause mortality”—meaning death from all causes put together—“and preventing chronic diseases such as coronary heart disease, stroke, diabetes, and cancer.” But don’t those diseases just run in our family? What if we just have bad genes?
According to the esteemed former chair of nutrition at Harvard, for most of the diseases that have contributed “importantly” to mortality in Western peoples, we’ve long known that non-genetic factors often account for at least 80% to 90% of risk. We know this because rates of the leading killers, like major cancers and cardiovascular diseases, vary up to 100-fold around the world, and, “when groups migrate from low- to high-risk countries, their disease rates almost always change to those of the new environment.” Modifiable behavioral factors have been identified, “including specific aspects of diet, overweight, inactivity, and smoking that account for over 70% of stroke and colon cancer, over 80% of coronary heart disease, and over 90% of adult-onset [type 2] diabetes”—diseases that can largely be prevented by our own actions.
If most of the power is in our own hands, why do we allocate massively more resources to treatment than prevention? And speaking of prevention, “even preventive strategies are heavily biased towards pharmacology rather than supporting improvements in diet and lifestyle that could be more cost-effective. For example, treatment of [high] serum cholesterol with statins alone could cost approximately 30 billion dollars per year in the United States and would have only a modest impact on coronary heart disease incidence. The inherent problem is that most pharmacologic strategies don’t address the underlying causes of ill health in Western countries, which are not drug deficiencies.”
Ironically, the chronic diseases that are most amenable to lifestyle treatment are the same ones most profitably treated by drugs. Why? If you don’t change your diet, you have to pop the pills every day for the rest of your life. So, the cash-cow drugs are the very drugs we need the least. “Even though the most widely accepted, well-established chronic disease practice guidelines uniformly call for lifestyle change as the first line of therapy, physicians often do not follow these recommendations.” “By ignoring the root causes of disease and neglecting to prioritize lifestyle measures for prevention, the medical community is placing people at harm.”
“Traditional medical care relies primarily on the application of pharmacologic and surgical interventions after the development of illness,” whereas lifestyle medicine relies primarily on “the use of optimal nutrition (a whole foods, plant-based diet) and exercise in the prevention, arrest, and reversal of chronic conditions leading to premature disability and death. It looks in a holistic way at the underlying causes of illness.”
Dr. Adriane Fugh-Berman, director of PharmedOut, a wonderful organization I’m proud to support, wrote a great editorial entitled “Doctors Must Not Be Lapdogs to Drug Firms.” “The illusion that the relationship between medicine and the drug industry is collegial, professional, and personal is carefully maintained by the drug industry, which actually views all transactions with physicians in finely calculated financial terms…The drug industry is happy to play the generous and genial uncle until physicians want to discuss subjects that are off limits, such as the benefits of diet or exercise, or the relationship between medicine and pharmaceutical companies…Let us not be a lapdog to Big Pharma. Rather than sitting contentedly in our master’s lap, let us turn around and bite something tender.”
Doctor’s Note
The organization I mentioned, PharmedOut, is a project of Georgetown University Medical Center.
For more on Lifestyle Medicine, see related videos below.
from NutritionFacts.org https://nutritionfacts.org/blog/treat-the-cause/
via IFTTT
Just a moment…
from Ob/Gyn & Women’s Health – Medscape https://www.medscape.com/viewarticle/doctors-5-deceptive-lab-tests-drop-better-options-2025a1000ttn
via IFTTT
Many Fear Federal Loan Caps Will Deter Aspiring Doctors and Worsen MD Shortage

Medical educators and health professionals are warning that new federal student loan caps could make it more expensive for many people to become doctors.
from Ob/Gyn & Women’s Health – Medscape https://kffhealthnews.org/news/article/medical-school-federal-loan-caps-doctor-shortage-trump-law/?utm_campaign=KHN:%20First%20Edition&utm_medium=email&_hsenc=p2ANqtz–fzqpUhpNHG0uqwj2-7CfA3IjPScJmQC2Vj9YcGIlcIP6KU_1MjCwfdh3uMp93LDFNdpyTcwfKTz7Ao1q7FR91
via IFTTT
Peter S. Bernstein, MD, MPH
from Ob/Gyn & Women’s Health – Medscape https://www.medscape.com/public/bios/ed-womenshealth#Bernstein
via IFTTT
Linda D. Bradley, MD
from Ob/Gyn & Women’s Health – Medscape https://www.medscape.com/public/bios/ed-womenshealth#Bradley
via IFTTT
Peter Kovacs, MD, PhD
from Ob/Gyn & Women’s Health – Medscape https://www.medscape.com/public/bios/ed-womenshealth#Kovacs
via IFTTT
JoAnn E. Manson, MD, DrPH
from Ob/Gyn & Women’s Health – Medscape https://www.medscape.com/public/bios/ed-womenshealth#Manson
via IFTTT
